Transcranial Magnetic Stimulation (TMS)
Repetitive Transcranial Magnetic Stimulation (rTMS)
Mental Illness Depression Brain Treatments

Summary:
In 1985 AD, Anthony Barker, proposed using Transcranial Magnetic Stimulation (TMS) to introduce electricity to the brain for medical treatment. Mark S. George began to apply this new method of shocking the brain to psychiatry in the treatment of depression, OCD and schizophrenia. The brain is an electric organ that runs on 1/10th of a single volt. TMS shocks the brain with 100 times that voltage through magnetic induction coils. "The most obvious and dangerous side effect of rTMS is the induction of epileptic seizures, and experience shows that currently available equipment is powerful enough to produce them readily." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 31) Repetitive Transcranial Magnetic Stimulation (rTMS) generates electricity about 2 inches inside the brain with electromagnets and is a milder, gentler form of ECT (Electro-convulsive shock therapy). The entire theory underlying TMS in psychiatry is a form of neo-phrenology, that wrongly believed different parts of the brain can be specifically mapped to single emotions or moods. TMS applies electricity to these "emotion centers" of the brain in an effort to modify those emotions. They use the exact language of phrenology, but in modern scientific terms: "localize functions within the human brain" "activation of selective mood circuits" "investigate brain mechanisms underlying specific emotions" "stimulation at different scalp locations derived largely from best-guess assumptions" They even admit the historical connection with phrenology: "TMS as a neuroscience probe fits within a historical current of attempting to localize functions within the human brain." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 31) This is pure junk science at its worst, since it was debunked over 200 years ago. Chemical psychiatrists reject the human spirit as a myth and therefore are forced to believe all emotion is the result of physical brain function and speak of "mood circuits". Before phrenology, Lavater's physiognomy, wrongly taught the shape of a persons skull determined their mental abilities. Christians can see the error of this thinking since the Bible says that emotions, will and choices have their origin in the human spirit, not the physical brain. TMS interrupts and disrupts normal brain function. TMS causes "lesions" in specific parts of the brain the size of a quarter (1 inch) which are like pressing the pause button on your music player for the duration of the shock. The procedure is entirely experimental and unproven. Only a few actual studies have been conducted, all of which are small, unscientific and unrepeatable in their conclusions. The therapeutic results are small and well within the error margin of the placebo effect: "Open studies with rTMS in depression have been compelling, but the possibility of placebo response must be kept in mind in interpreting these results, given that smaller effect sizes have generally been observed in controlled, blinded trials." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 133) If TMS, or any brain shocking psychiatric therapy would be effective, it would be important to be able to map the regions of the brain for individual emotions. This has been tried and tried and tried over and over and over again... and there is no direct correlation between the parts of the brain and emotions, thoughts etc. Changes in blood flow in part of the brain that are shocked have been reported: "neural response to TMS correlated directly to changes in blood flow to the region." (Neural Activity Connected To Blood Flow In New Brain Stimulation Technique, Science Daily, Oct. 11, 2007) However, similar changes in blood flow are reported in you finger, when you stick it in a light socket and get a shock. The idea of blood flow related to the cause and cure of insanity is a throw back to our "hero of modern psychiatry" Benjamin Rush, who taught in 1812 AD that insanity was caused by bloated blood vessels: "the cause of madness is seated primarily in the blood-vessels of the brain". TMS is pure junk-pop psychiatry at its worst and millions of dollars are being wasted in research! Applying electricity to the brain to affect emotion is like hitting the USB cable that connects your computer to the printer with a hammer and expecting some improvements in print quality. (Repetitive Transcranial Magnetic Stimulation, rTMS)
"But the more lucrative application for DBS is as a treatment for refractory depression rather than OCD. As of late 2006, a number of groups are chasing success in this area. Unlike OCD, however, there is no consensus on what brain circuitry is affected in depression, and without such accord, many question whether the hazards of this treatment are worth pursuing for a condition that can often clear up miraculously without treatment. DBS may well offer benefits, but efforts to develop it, at least for depression, have the potential to inflict the kind of damage on psychiatry's current stock of physical therapies that psychosurgery inflicted in the 1950s, bringing the whole field to a standstill once more." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 283)
Introduction:
Transcranial Magnetic Stimulation (TMS) is utterly worthless in the treatment of depression or any so called mental illness apart from the placebo effect. The therapeutic results small and well within the error margin of the placebo effect: "Open studies with rTMS in depression have been compelling, but the possibility of placebo response must be kept in mind in interpreting these results, given that smaller effect sizes have generally been observed in controlled, blinded trials." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 133)
In short, is it a form of neo-phrenology, that wrongly believes different parts of the brain can be specifically mapped to single emotions. TMS applies electricity to these "emotion centers" of the brain in an effort to modify those emotions. This is pure junk science at its worst, since it was debunked over 200 years ago. Before this, Lavater's physiognomy, taught the shape of a persons skull determined their mental abilities.
 TMS and "Repetitive Transcranial Magnetic Stimulation" (rTMS) are ways of generating electricity about 2 inches inside the brain with electromagnets and is a milder, gentler form of ECT (Electro-convulsive shock therapy).
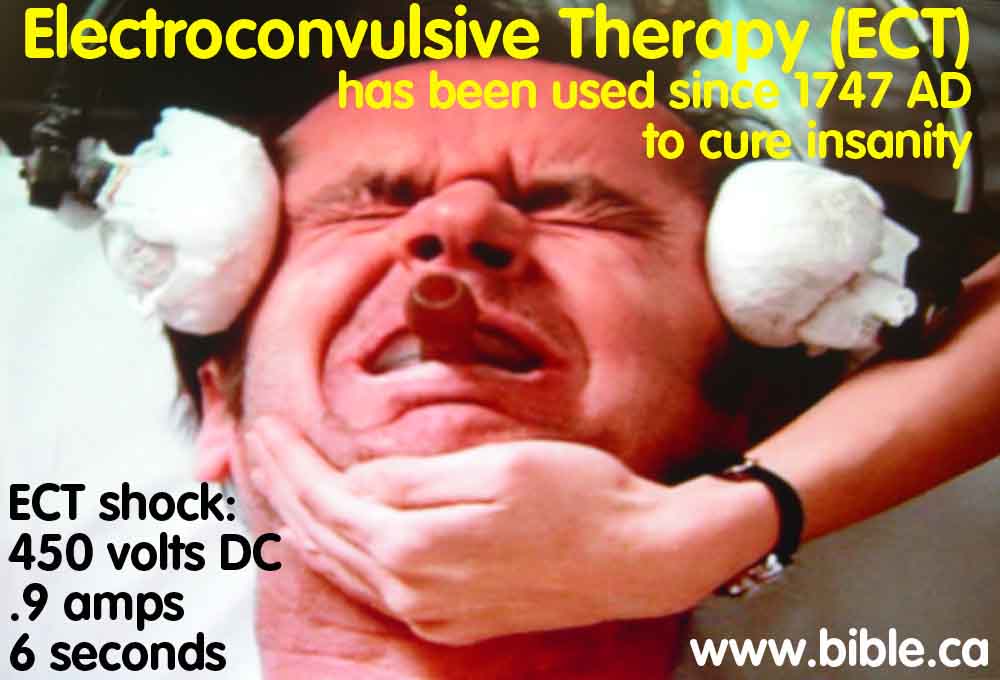
There are several ways of getting electricity inside the brain. First, Electro-convulsive shock therapy that takes two wires and puts .9 amps at 450 volts DC for 6 seconds directly on the skull, enough to an 84 watt light bulb. Anybody who has taken a high school introductory course on electricity knows this is more than enough to burn and kill living brain tissue. TMS differs from ECT in that it can pinpoint where the electricity is generated in an area the size of a quarter. 2 inches below the skull. Second, Deep brain stimulation. Third, TMS through magnetic induction.
TMS and "Repetitive Transcranial Magnetic Stimulation" (rTMS) are ways of generating electricity about 2 inches inside the brain with electromagnets and is a milder, gentler form of ECT (Electro-convulsive shock therapy).
There are several ways of getting electricity inside the brain. First, Electro-convulsive shock therapy that takes two wires and puts .9 amps at 450 volts DC for 6 seconds directly on the skull, enough to an 84 watt light bulb. Anybody who has taken a high school introductory course on electricity knows this is more than enough to burn and kill living brain tissue. TMS differs from ECT in that it can pinpoint where the electricity is generated in an area the size of a quarter. 2 inches below the skull. Second, Deep brain stimulation. Third, TMS through magnetic induction.
 TMS is a method of inducing man made seizures with electricity applied to the brain like ECT, but on smaller scale. Whereas ECT sends the entire body in one massive convulsion, TMS is scaled back to just below the level that your index finger will involuntarily twitch. "The most obvious and dangerous side effect of rTMS is the induction of epileptic seizures, and experience shows that currently available equipment is powerful enough to produce them readily." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 31)
Another way of generating the same amount of electricity as TMS, in the same small targeted area of the brain the size of a quarter, 2 inches deep, is to push two insulated electrodes physically into the brain and flip the wall switch! This is being done with Deep brain stimulation, 6 inches inside the brain! But this would cause physical damage to the brain with two puncture wounds. Herein lies the advantage of TMS because it does no apparent physical tissue damage.
The brain is an organ that generates and transmits commands to the body with 1/10th of a volt of electricity. It has been known for some time, that if you apply electricity to certain parts of the brain, you can make the index fingers twitch, or make some muscles contract involuntarily. This should not surprise us since the brain sends electricity through the spinal cord to the muscles as a normal function. "Intracellular Charge: All living cells possess an electrical charge, with the inside of the cell more negatively charged than the outside (Rosenzweig et al. 2005). The resting membrane potential in a nerve cell is approximately 50 to 80 millivolts. [50-80/1000] Nerve cells use this property to communicate with one another." (Brain Stimulation Therapies For Clinicians, Deep Brain Stimulation in Neurological and Psychiatric Disorders, E. Higgins, M. George, 2009 AD)
The reason TMS is utterly worthless as a treatment for depression, is because there has never been a case where emotions have been involuntarily created when zapping a part of the brain with electricity. It is really that simple. Imagine moving the TMS magnet over the skull and a person starts being happy, then sad, then... as the magnet moves... becomes angry... or amorous, or aggressive. This is what pop-psychiatrists imagine is happening and what they hope in vain to someday discover. It is like trying to understand Windows software by looking at the physical mother board of your computer.
Of course Christians understand that man has a spirit that is distinct from his body. The Christian understands from the Bible story of Luke 16:19-31, that when we die and our brain becomes dust, that we retain our memories, will, desires and emotions. Depression is a spiritual problem, not a physical disease.
"Transcranial magnetic stimulation (TMS) is a method that relies on a short-lived magnetic field which is induced by a high current (approx. 5000 Amp) running through a well insulated cable wound into a coil. This field lasts for about half a millisecond and reaches peak amplitudes of 3 Tesla, which is comparable to the field strength used in MRI scanning. Neurons react to these extreme magnetic fluctuations (rising from 0 to 3 Tesla and back to 0 within less than a millisecond) by producing signaling impulses themselves. If the coil, being relatively small and lightweight, is placed to the head of the subject, the nerve cells just underneath the focus of the coil send impulses synchronous to the TMS pulse (normally up to once a second). Since this simultaneous firing of complete neural populations is without any functional content, information processing in this part of the brain is disturbed for fractions of a second. This allows us to induce "virtual lesions", i.e. simulate the failure of the brain region in question without jeopardizing the subject. By deliberately integrating TMS in a well elaborated experiment, one can prove the importance of the brain part in a given cognitive function because performance deficits can be expected. To optimize targeting during TMS experiments, previously obtained (functional) MR imaging data can be utilized for the so called neuro-navigation. A computer compares the brain scan with the subject's head and thus enables a very precise positioning of the coil on the head, just over the brain region of interest. Magnetic field strength: 0,5 - 3,5 Tesla. Maximum repetition rate: 50 Hz bei 30% max. stimulator output. 30 Hz bei 50%. 18 Hz bei 80%. 15 Hz bei 100%. In our experiments, we normally use stimulation frequencies of 1Hz, and sometimes short pulse series of 10Hz. Duration of a single impluse: 400µs." (Max Planck Institute for Human Cognitive and Brain Sciences)
TMS is a method of inducing man made seizures with electricity applied to the brain like ECT, but on smaller scale. Whereas ECT sends the entire body in one massive convulsion, TMS is scaled back to just below the level that your index finger will involuntarily twitch. "The most obvious and dangerous side effect of rTMS is the induction of epileptic seizures, and experience shows that currently available equipment is powerful enough to produce them readily." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 31)
Another way of generating the same amount of electricity as TMS, in the same small targeted area of the brain the size of a quarter, 2 inches deep, is to push two insulated electrodes physically into the brain and flip the wall switch! This is being done with Deep brain stimulation, 6 inches inside the brain! But this would cause physical damage to the brain with two puncture wounds. Herein lies the advantage of TMS because it does no apparent physical tissue damage.
The brain is an organ that generates and transmits commands to the body with 1/10th of a volt of electricity. It has been known for some time, that if you apply electricity to certain parts of the brain, you can make the index fingers twitch, or make some muscles contract involuntarily. This should not surprise us since the brain sends electricity through the spinal cord to the muscles as a normal function. "Intracellular Charge: All living cells possess an electrical charge, with the inside of the cell more negatively charged than the outside (Rosenzweig et al. 2005). The resting membrane potential in a nerve cell is approximately 50 to 80 millivolts. [50-80/1000] Nerve cells use this property to communicate with one another." (Brain Stimulation Therapies For Clinicians, Deep Brain Stimulation in Neurological and Psychiatric Disorders, E. Higgins, M. George, 2009 AD)
The reason TMS is utterly worthless as a treatment for depression, is because there has never been a case where emotions have been involuntarily created when zapping a part of the brain with electricity. It is really that simple. Imagine moving the TMS magnet over the skull and a person starts being happy, then sad, then... as the magnet moves... becomes angry... or amorous, or aggressive. This is what pop-psychiatrists imagine is happening and what they hope in vain to someday discover. It is like trying to understand Windows software by looking at the physical mother board of your computer.
Of course Christians understand that man has a spirit that is distinct from his body. The Christian understands from the Bible story of Luke 16:19-31, that when we die and our brain becomes dust, that we retain our memories, will, desires and emotions. Depression is a spiritual problem, not a physical disease.
"Transcranial magnetic stimulation (TMS) is a method that relies on a short-lived magnetic field which is induced by a high current (approx. 5000 Amp) running through a well insulated cable wound into a coil. This field lasts for about half a millisecond and reaches peak amplitudes of 3 Tesla, which is comparable to the field strength used in MRI scanning. Neurons react to these extreme magnetic fluctuations (rising from 0 to 3 Tesla and back to 0 within less than a millisecond) by producing signaling impulses themselves. If the coil, being relatively small and lightweight, is placed to the head of the subject, the nerve cells just underneath the focus of the coil send impulses synchronous to the TMS pulse (normally up to once a second). Since this simultaneous firing of complete neural populations is without any functional content, information processing in this part of the brain is disturbed for fractions of a second. This allows us to induce "virtual lesions", i.e. simulate the failure of the brain region in question without jeopardizing the subject. By deliberately integrating TMS in a well elaborated experiment, one can prove the importance of the brain part in a given cognitive function because performance deficits can be expected. To optimize targeting during TMS experiments, previously obtained (functional) MR imaging data can be utilized for the so called neuro-navigation. A computer compares the brain scan with the subject's head and thus enables a very precise positioning of the coil on the head, just over the brain region of interest. Magnetic field strength: 0,5 - 3,5 Tesla. Maximum repetition rate: 50 Hz bei 30% max. stimulator output. 30 Hz bei 50%. 18 Hz bei 80%. 15 Hz bei 100%. In our experiments, we normally use stimulation frequencies of 1Hz, and sometimes short pulse series of 10Hz. Duration of a single impluse: 400µs." (Max Planck Institute for Human Cognitive and Brain Sciences)
|
|
"An electromagnetic coil is placed against your scalp on an area near your forehead, often on the left side. To produce the stimulating pulses, the electromagnetic coil is switched off and on repeatedly, sometimes up to 10 times a second. This results in a tapping or clicking sound that usually lasts for a few seconds, followed by a pause. You'll also feel a light tapping sensation on your forehead. This part of the process is called "mapping." Your "motor threshold" will be determined. This is the minimum amount of energy needed to make your fingers or hands twitch. The coil is adjusted until the right setting is found." (Mayoclinic, 2010) |
A. rTMS is experimental, speculative and unproven!
Nobody knows the cause or cure of any mental illness including schizophrenia! Causes are always stated in terms like "we think", meaning that it is 100% theoretical and unproven in real science. The claims for TMS as a treatment for mental illnesses are always stated in speculative, hopeful terms. Notice in the statement below the words in blue: This is clearly a statement of faith unworthy of the real scientific arena where real live humans are being experimented upon by psychiatrists.
"How it works: It's not clear precisely how transcranial magnetic stimulation may help relieve symptoms of depression. Networks of brain regions may play a role in mood regulation. Stimulating the brain in these regions may change how the brain functions and may lead to mood improvement. ... When transcranial magnetic stimulation works: If transcranial magnetic stimulation works for you, your depression symptoms could improve or go away completely. This improvement, if it occurs, may be gradual and take a few weeks. Improvement in your mood may last for days or weeks. Some research, however, shows a lack of dramatic improvement in depression symptoms. But as researchers learn more about different techniques, the number of stimulations required and the best sites on the brain to stimulate, the effectiveness of transcranial magnetic stimulation may improve over time." (Mayoclinic, 2010)
"Although studies of TMS in depression are now proliferating, the initial idea that this intervention might be effective in major depression went against clinical dogma in the field of electroconvulsive therapy (ECT). The tenet that a seizure is necessary but not sufficient for ECT to exert antidepressant effects is now widely accepted (Sackeim et al. 1993). Subconvulsive electrical stimulation has long been known to be ineffective in depression (Fink et al. 1958), and thus it seemed unlikely that electrical stimulation induced in the brain via TMS would behave differently than the direct application of electricity transcranially. On closer investigation, however, TMS and subconvulsive ECT bear little resemblance to each other as somatic interventions." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 121)
"It appears that neither psychiatrists, nor the editors of medical and scientific publications, nor the media, nor the public feel the need to reconcile the contradiction of treating the same brain disease with interventions as different as ECT, VNS, DBS, TMS, antidepressant drugs, cognitive therapy, various "talk therapies," and dolphin therapy. At this point, it may be well to recall that the so-called effectiveness of this kind of therapeutic hocus-pocus had been investigated more than two hundred years ago by some of the greatest scientific figures of the time who had no difficulty concluding that the miracle-cure they were examining—Mesmerism—was simply bogus. Just as importantly, they also concluded that because healer and healed are equally deceived and self-deceived, the effectiveness of the hocus-pocus therapy appears real, at least for a while. Then, after they are debunked, they lose their effectiveness and are soon replaced by new miracle cures. Mesmer first used magnets to cure patients. Then his mere touch turned out to be curative. Finally, he didn't even have to touch patients to cure them—they could cure themselves and each other by means of rituals that utilized the powers of an imaginary magnetic fluid, a property of "animal magnetism." Between 1774 and 1777, in a mere three years, Mesmer rose from obscure physician to world-famous healer, only to be exposed as a quack." (Coercion as Cure, Thomas Szasz, 2007 AD, p 148)
TMS cannot help depression because emotion originates with the spirit, not the body. The brain is the interface between the body and the spirit. Applying electricity to the brain to affect emotion is like trying hitting the USB cable that connects your computer to the printer with a hammer and expecting some improvements in print quality.
B. Studies are small, short in duration, not blind and unreplicated:
"Alvaro Pascual-Leone, working at NIH on TMS with Hallett and Wassermann at the same time as George, had returned to his native Spain, and in short order, he recruited a group of psychotically depressed subjects to a study in which high-frequency left prefrontal rTMS was compared to sham TMS. The results reported in the Lancet showed that in seventeen patients with medication-resistant psychotic depression—the severest kind of depression—there were dramatic responses after a week of treatment. "Our findings emphasize the role of the left dorsolateral prefrontal cortex in depression and suggest that rTMS of the left dorsolateral prefrontal cortex might become a safe, non- convulsive alternative to electroconvulsive treatment in depression."" ... "But all was not as it seemed. The first problem was that Pascual-Leone's research, rushed to publication in the Lancet in 1996, turned out to be mysteriously unreplicable. No one else has been able to show a comparable response in psychotic depression, especially on the time-scale of a week. Although researchers from Germany to Japan and from Brazil to Canada attempted to reproduce the results of this study, all have achieved negative results. ... The bubble burst, however, when from within the field of rTMS research, Thomas Schlaepfer and others meta-analyzed the body of published studies as of 2003 (limiting their analysis to those studies with reasonable protocols and where results were adequately reported), and concluded that "current trials are of low quality and provide insufficient evidence to support the use of rTMS in the treatment of depression."" TMS appeared to have some effect on mood, but it was not significant enough to replace anything in the therapeutic armamentarium, and certainly not ECT." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 263, 269)
"The body of literature on the use of TMS in depression is rapidly growing, and many of the findings have been encouraging. ... It is important to note several limitations in the cited studies. Perhaps most importantly, none of the key findings have been rigorously replicated. Most studies included small sample sizes making it harder to detect effects. Nearly all of the published trials were of a short trial duration compared with psychopharmacological trials, and to date there has been only a few published works on continuation or maintenance treatments." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 142)
"In summary, these studies suggest that schizophrenia is associated with reduced cortical inhibition in the motor cortex, although findings are not always replicated clearly across studies. Motor threshold appears to demonstrate enhanced cortical excitability in schizophrenia, especially on the left side." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 185)
"Open studies with rTMS in depression have been compelling, but the possibility of placebo response must be kept in mind in interpreting these results, given that smaller effect sizes have generally been observed in controlled, blinded trials." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 133
C. rTMS is Neo-phrenology:
rTMS is it a form of neo-phrenology, that wrongly believes different parts of the brain can be specifically mapped to single emotions. TMS applies electricity to these "emotion centers" of the brain in an effort to modify those emotions. This is pure junk science at its worst, since it was debunked over 200 years ago. Before this, Lavater's physiognomy, taught the shape of a persons skull determined their mental abilities. TMS continues this quacky junk science today and it is shameful.
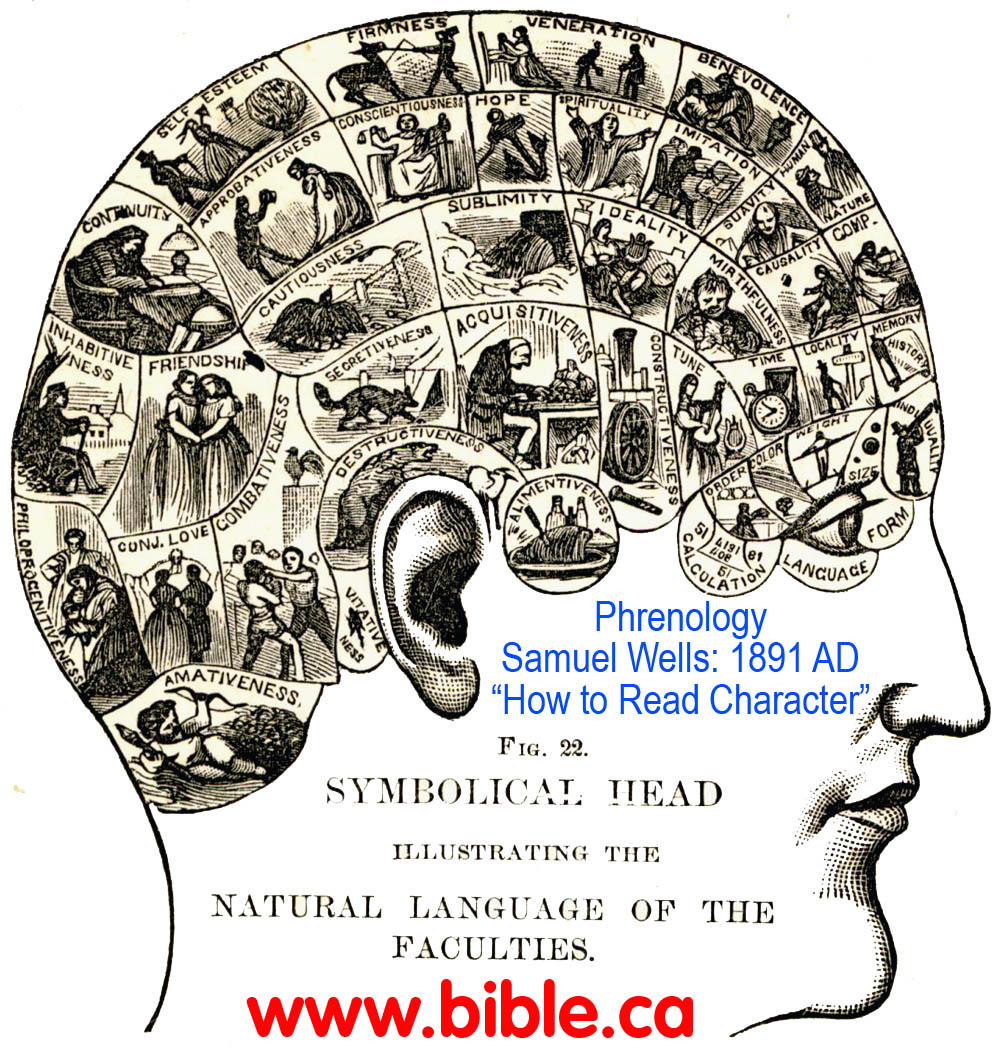 Although magnets and Phrenology were popularized by Samuel Wells in as late as 1891 AD, chemical psychiatry has no where else to look for the cause of insanity. Notice that they continue to believe the myth that emotion is localized in specific brain circuits. Take note of the language they use:
Although magnets and Phrenology were popularized by Samuel Wells in as late as 1891 AD, chemical psychiatry has no where else to look for the cause of insanity. Notice that they continue to believe the myth that emotion is localized in specific brain circuits. Take note of the language they use:
"localize functions within the human brain"
"activation of selective mood circuits"
"investigate brain mechanisms underlying specific emotions"
"stimulation at different scalp locations derived largely from best-guess assumptions"
This is pure Phrenology!
"But the more lucrative application for DBS is as a treatment for refractory depression rather than OCD. As of late 2006, a number of groups are chasing success in this area. Unlike OCD, however, there is no consensus on what brain circuitry is affected in depression, and without such accord, many question whether the hazards of this treatment are worth pursuing for a condition that can often clear up miraculously without treatment. DBS may well offer benefits, but efforts to develop it, at least for depression, have the potential to inflict the kind of damage on psychiatry's current stock of physical therapies that psychosurgery inflicted in the 1950s, bringing the whole field to a standstill once more." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 283)
"TMS as a neuroscience probe fits within a historical current of attempting to localize functions within the human brain. As a potential therapy, TMS follows on the heels of ECT, although since its very beginning there have been important differences between these two techniques. TMS is emerging at a time of renewed popular interest in magnets and healing." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 31)
"Mark George studied medicine at the University of South Carolina and then secured a place at NIMH. Convinced that most psychological syndromes would turn out to be brain circuit disorders, George was intent on training in both neurology and psychiatry. ... But George's early work on neuro-imaging was just then starting to take focus, pointing to a more dynamic and important role for traditionally more quiescent areas of the brain such as the prefrontal cortex. Positron emission tomography (PET) scans and magnetic resonance imagery (MRI) revealed activity in brain tissue in a completely new way, suggesting underactive and overactive brain circuits played a role in conditions from Parkinson's disease to obsessive-compulsive disorder (OCD)." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 259)
"Besides the stimulation with a large, non- focal, round coil, many of these studies involved different positioning of TMS applications over the vertex, choosing multiple sites in the same patient, so speculation about activation of selective mood circuits is difficult. ... TMS comparing coil size and stimulation site will be needed to clarify if this form of stimulation will be clinically useful, even if the application of the repetitive form of TMS seems nowadays the most promising treatment." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 132)
"Other kinds of TMS research might contribute to our understanding of physiological or regional correlates of factors predisposing to development of anxiety disorders. ... Another intriguing use of TMS is to investigate brain mechanisms underlying specific emotions, including those elicited in a situationally specific manner, which is a common feature of anxiety disorders. For instance, rTMS research in healthy subjects suggests that the emotions anger and anxiety are lateralized in the prefrontal cortex." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 174)
"Priorities for research on TMS in the near future: In general, the main TMS methods of delivery remain unexamined, following protocols in early studies that found antidepressant efficacy (George et al. 1995, 1997). Thus, it is unclear whether stimulation at different scalp locations, with different use parameters or dosing strategies or with different coils (Roth et al. 2002, 2005), will affect clinical outcomes. The TMS use parameters, derived largely from best-guess assumptions, are expensive and slow to work out in clinical trials. Thus, a key step for TMS clinical advancement would be to develop quick- change, laboratory-based measures that relate to ultimate antidepressant response. TMS has rapidly progressed from an interesting technique, outside of most paradigms, to an FDA-approved treatment for depression. It will likely not be restricted to use in depression for long." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 262)
"One of the images [PET, MRI] that came into focus was that of the depressed brain, where it seemed there was reduced activity in the prefrontal lobes and an underlying pathology in the frontal lobes themselves or in the basal structures of the brain that interconnected with the frontal areas. If some treatment could be found that stimulated activity in these areas, it might turn out to be a cure for depression. Perhaps this was the mechanism by which ECT had its effect—the current in bilateral ECT is, after all, directed through the prefrontal lobes." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 260)
"Guided by brain images that showed hyperactivity in what appeared to be a discrete brain circuit, they attempted to treat OCD with TMS by interfering with specific circuits rather than stimulating the brain as a whole." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 262)
"In contrast, rTMS, for instance, appeared to be as rational a treatment as could be wished for. George had linked TMS usage to an effort to alter blood flow through the prefrontal cortex in a manner that would reverse psychiatric symptoms ascribed to this area. Increasing the dose appeared to have a bigger effect on changes in blood flow, opening up the possibility of establishing TMS as a highly rational and predictable treatment option." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 268)
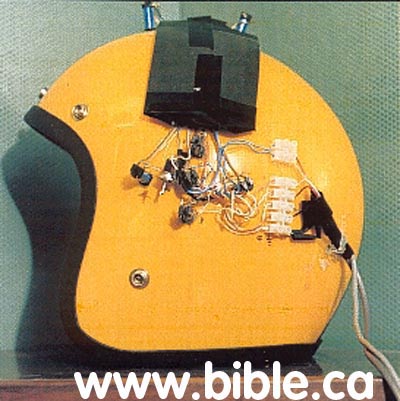
Junk Pop psychiatrists are always in the market for a new treatment. They have a long list of failed treatments that have been discontinued. Psychiatrists are hopeful that rTMS will cure not only depression, but every form of insanity. But there is a big problem with their idea. While it is true that zapping the brain in position X will make your finger twitch or a muscle contract, they have never induced emotion. We are reminded of "The God helmet" invented in 2002 by Junk Pop psychologist Michael Persinger, to induce a spiritual experience into the brain with magnetism applied to the brain. Even atheist Richard Dawkins embarrassed himself by flying 7000 miles to try it on and experience God for himself! He felt nothing. ... Wait a few decades, Richard, one day you will have a genuine spiritual experience!
D. Blood flow in the brain:
The idea that insanity was caused by "bloated blood vessels" or abnormal blood flow in the brain has a long quacky history in theoretical psychiatry.
"What the researchers were able to determine for the first time was that the neural response to TMS correlated directly to changes in blood flow to the region. Using oxygen sensors and optical imaging, the researchers found that an initial increase in blood flow was followed by a longer period of decreased activity after the magnetic pulses were applied. ... The critical confirmation of the connection between blood flow and neural activity means that researchers can use TMS to alter neural activity, and then use fMRI, which tracks blood flow changes, to assess how the nerve cells respond over time." (Neural Activity Connected To Blood Flow In New Brain Stimulation Technique, Science Daily, Oct. 11, 2007)
Our "hero of modern psychiatry" Benjamin Rush, taught in 1812 AD that insanity was caused by bloated blood vessels: "the cause of madness is seated primarily in the blood-vessels of the brain" (Medical Inquiries and Observations Upon the Diseases of the Mind, Benjamin Rush 1812 AD)
 Since psychiatry has made no scientific advancement in 200 years, this old idea has been resurrected as the cause of insanity. It was wrong in 1812 and it is still wrong today!
Similar changes in blood flow are reported in you finger, when you stick it in a light socket and get a shock. We would have predicted that the brain would have an altered blood flow when you shock it with 100 x higher voltage than it normally runs on. What passes for science today is "shocking".
Since psychiatry has made no scientific advancement in 200 years, this old idea has been resurrected as the cause of insanity. It was wrong in 1812 and it is still wrong today!
Similar changes in blood flow are reported in you finger, when you stick it in a light socket and get a shock. We would have predicted that the brain would have an altered blood flow when you shock it with 100 x higher voltage than it normally runs on. What passes for science today is "shocking".
E. VBS disrupts normal brain function: "Lesions"
When VBS shocks the vagus nerve, it disrupts normal brain function. This really is no surprise to any one who took the grade 9 introductory electricity course. In technical terms, this disruption is called a "lesion".
There is a lot of talk about TMS inducing "virtual lesions" in the brain which "simulate the failure of the brain region in question without jeopardizing the subject".
Lesioning is like when your computer freezes for a moment during a power surge. All activity in the CPU stops while the power surge occurs. When the surge is over the CPU picks up where it left off.
Electrical lesioning fixes a fibrillating heart. Arrhythmia is when the heart beats in an irregular or spasmodic rhythm. Atrial fibrillation occurs when the heart's electrical system makes the atria to quiver or "fibrillate". Different parts of the heart beat at different rates which means blood is no longer being pumped efficiently. The solution is a heart "Defibrillator" which we have all seen in emergency wards where the nurse puts two electrode paddles over the heart and on the side of the chest. "All clear", then zap! The shock makes the body jump off the bed, but the heart beat is reset back to normal rhythm. The is a prefect example of how electricity creates a lesion and saves a person's life. Applying "defibrillator" theory to correcting emotions by shocking the brain, is completely different matter and doesn't work.
"As with TMS, DBS depends on neuro-imaging technology. In order to implant the electrodes in the correct location, it is necessary to be able to map each patient's brain in great detail using both MRI and CT scans, fusing these with computer programs to get a precise fix on the path of nerve tracts and blood vessels. A misplaced electrode can cause hemorrhage and death. The 2004 remake of The Manchurian Candidate gives a reasonably accurate image of what the procedure looks like. When the electrodes are in place, a battery operated device produces a stimulation that can be increased or decreased in frequency based on feedback from the patient. This stimulation can theoretically work by either overstimulating nerve cells, leading to somatic fatigue, or jamming the nerve cells so signals do not get through, in either case producing a functional lesion." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 281)
We do not question the factual nature of these virtual lesions... and why would we. If you have ever watched ECT, where 450 volts is directly applied through the brain, you can imagine that the "patients ability to count backwards in increments of 13 is seriously impaired". The smaller amounts of electricity induced through rTMS would have a proportional effect.
rTMS makes the junk pop-psychiatry O-meter goes crazy!
 (Left: Junk pop-psychiatry O-meter going crazy)
The application of rTMS to depression is entirely theoretical and unproven.
(Left: Junk pop-psychiatry O-meter going crazy)
The application of rTMS to depression is entirely theoretical and unproven.
F. Hopeful "Cure all" for all mental illness:
Step right up and buy some of Dr. Mark George's cure for: schizophrenia, depression, anxiety disorders, Obsessive compulsive disorder (OCD), Tourette's syndrome, posttraumatic stress disorder (PTSD)!!!
|
 |
"Although TMS will be approved for the treatment of depression, it is probable that clinicians will rapidly begin using it for other disorders. The best evidence to date exists for its use in acute pain syndromes (Borckardt et al., in press), hallucinations in schizophrenia, and anxiety disorders, particularly OCD." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 262) |
- "Although one would be justified in greeting with amusement, if not ridicule and derision, some of the speculations in this chapter about the future uses of rTMS, one need only look at the exponential explosion in neuroscience knowledge in the latter part of the twentieth century to envision the possibility of dramatic therapeutic interventions in the near future." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 247)
- "The authors' conclusion that low-frequency rTMS of the right prefrontal cortex failed to produce significant improvement of OCD is of interest in light of another report that short- term TMS (2 days) at 1 Hz failed to affect either obsessions, compulsions, or tics in patients with Tourette's syndrome in a sham-controlled, crossover study (Munchau et al. 2002). The conclusion remains that further studies are indicated to assess the efficacy and to clarify the optimal stimulation characteristics of rTMS in OCD." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 172)
- "There is some preliminary research on therapeutic effects of TMS in posttraumatic stress disorder (PTSD). ... Recent theories of PTSD pathogenesis suggest that mechanisms involved in normal threat assessment become dysregulated so that fear responses associated with the original traumatic situation become overgeneralized and fail to extinguish (Rauch et al. 1997). This model makes the commonsense proposal that brain regions associated with fear conditioning and extinction are important in PTSD. ... For the purposes of this review, it is most important to note that limbic and paralimbic activation appears associated with traumatic memory—related anxiety, and prefrontal input could modulate PTSDrelated subcortical activity." (Transcranial magnetic stimulation in clinical psychiatry, Mark S. George, Robert H. Belmaker, 2007 AD, p 173)
Conclusion:
The Christian knows that depression and insanity happens in the spirit, not the physical body. The error of chemical psychiatrists, is rooted in their atheistic belief in evolution where man is viewed as nothing more than a pile of chemicals and electrons. They openly mock Christians who view the nature of man is dichotomous, having a distinct body and soul.
This error has dead ended psychiatric research into insanity in the physical brain as the etiological cause of insanity for 300 years. rTMS is neo-Phrenology and carries forward the error that insanity is rooted in the physical brain and somehow related to blood flow within the cortex and dura mater. "It is not important whether this cerebroversion hypothesis is correct; the point is to highlight modern psychiatry's failure of imagination. At the start of the twenty-first century, thinking has been dominated by "bio-babble," a discourse characterized by jargon and an emphasis on the monoamines, dopamine, serotonin, and norepinephrine. Within a few years, this will almost certainly seem as vacuous as Freudian notions about libido. The problem, in the meantime, is that just as psychoanalysis once inhibited a generation from making progress in understanding what mental disorders are, so too psychopharmacology has held back development in theoretical aspects of psychiatry, at the expense of patients." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 296)
TMS and rTMS have some important applications to mapping the brain to physical functions, like which part of the brain controls your index finger etc. However there is no way to map emotions to specific parts of the brain. The brain does not contain "mood circuits" that create and generate emotion. Rather the brain is the physical organ that connects the body to the spirit in the same way a USB cable connects a computer to the printer.
TMS is the "new kid on the street" that is has captured researchers attention to find some treatment for schizophrenia, depression, anxiety disorders, Obsessive compulsive disorder (OCD), Tourette's syndrome, posttraumatic stress disorder (PTSD). However, at present, there is no evidence TMS has any more effect on curing depression, or any mental illness, than might be expected as the placebo effect.
"Time will tell whether another chapter in the history of shock therapy is being written today or not. The history of the past sixty years has been a history of successive attempts to improve ECT. All have failed, even if individual lives were helped along the way. The treatment that Cerletti described in 1938, plus a few modifications involving muscle relaxation and wave form, is still with us today, and a row of bright ideas about magnets, nonconvulsive applications of electricity, and the like have not succeeded in making patient care better or safer. It remains to be seen if the current therapies will provide more convincing alternatives." (Shock Therapy: A History of Electroconvulsive Treatment in Mental Illness, Edward Shorter, David Healy, 2007, p 289)
TMS is pure junk science at its worst and it is a harmful treatment because if applies voltages 100 times higher than what the brain normally uses. Think of the damage that would be done to using house current to jump start your car.... that is only 10 times the voltage. Shocking to brain to change emotions is stupid junk science, but biologic psychiatrists have no other place to look for the cause of insanity. Christians have God's word to give us the answers we seek, that emotion, thought, mood and memory happen in the spirit, not the body. (see Luke 16:19-31)
By Steve Rudd:
Contact the author for comments, input or corrections.
Send us your story about your experience with modern Psychiatry
Go To Start: WWW.BIBLE.CA